Jerold S Bell, DVM
Cummings School of Veterinary Medicine at Tufts University, N. Grafton, MA
Polygenic disorders have been difficult for breeders to control. Examples are hip dysplasia, congenital heart defects, and epilepsy. Controlling polygenically inherited disorders involves; 1) identifying traits that more closely represent genes being selected against, 2) the standardization of nuisance factors (such as environment) that can limit your selective pressure against the genes and 3) selecting for breadth of pedigree as well as depth of pedigree.
Hip dysplasia is a classic example of a polygenically controlled hereditary disease. Due to genetically controlled defects in anatomy and/or joint laxity, affected dogs can become lame, and eventually crippled due to secondary osteoarthritis. The genetic test used to control hip dysplasia is the pelvic radiograph (x-ray).
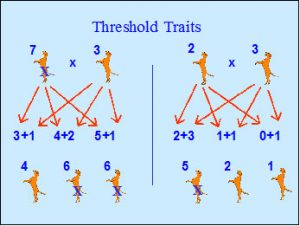 To control polygenic disorders, they must be considered as threshold traits. A number of genes must combine to cross a threshold producing an affected individual. Genes that combine in an additive manner are considered quantitative genes. If we theoretically state that five quantitative genes contributing to hip dysplasia can produce a dysplastic dog, then dogs receiving less than five genes from their parents would have normal hips. If phenotypically normal parents produce affected offspring, both should be considered to carry a genetic load that combined to cause the disorder.
To control polygenic disorders, they must be considered as threshold traits. A number of genes must combine to cross a threshold producing an affected individual. Genes that combine in an additive manner are considered quantitative genes. If we theoretically state that five quantitative genes contributing to hip dysplasia can produce a dysplastic dog, then dogs receiving less than five genes from their parents would have normal hips. If phenotypically normal parents produce affected offspring, both should be considered to carry a genetic load that combined to cause the disorder.
Many polygenic disorders have a major recessive or dominant trigger gene that must be present to produce an affected individual. Genes that act in a dominant or recessive manner are considered qualitative genes. If qualitative genes play a role in hip dysplasia, then it is possible that dogs with more than the threshold of quantitative genes could be phenotypically normal if they do not carry a qualitative trigger gene. They would pass on a high liability for dysplasia through their contributing high numbers of the additive genes.
A trigger gene in one breed or family may be different from the gene in others. Consequently, if a test for a trigger gene is developed in one breed or family, it may not provide useful information for all breeds or families. Molecular genetic research to identify major qualitative disease causing genes can allow better control of polygenic disorders such as hip dysplasia, epilepsy, and cataracts.
Breeders must break down hip phenotypes into traits that more directly represent the genes that control them.
 One reason we have not had great progress with hip dysplasia control is that it is being treated as a single gene disease, with a test for carriers. There is no excellent hip gene, although that is what most breeders are selecting for. In polygenic disorders, the phenotype of the individual does not directly represent its genotype. Breeders must break down affected phenotypes into traits that more directly represent the genes that control them. These include clinical signs of lameness (especially during the critical period of bony ossification between six and eighteen months of age), palpable laxity under anesthesia, deep acetabula, rounded femoral heads, the absence of remodeling, deeply seated hips on an extended leg view, and radiographic distractibility.
One reason we have not had great progress with hip dysplasia control is that it is being treated as a single gene disease, with a test for carriers. There is no excellent hip gene, although that is what most breeders are selecting for. In polygenic disorders, the phenotype of the individual does not directly represent its genotype. Breeders must break down affected phenotypes into traits that more directly represent the genes that control them. These include clinical signs of lameness (especially during the critical period of bony ossification between six and eighteen months of age), palpable laxity under anesthesia, deep acetabula, rounded femoral heads, the absence of remodeling, deeply seated hips on an extended leg view, and radiographic distractibility.
We know that the environment has a role in the expression of hip dysplasia. Overnutrition and excessive environmental trauma during the critical growth periods prior to skeletal maturation will promote later dysplastic development. While limiting these environmental stresses is prudent in pet dogs, it is recommended that breeders do not overly protect or overly stress prospective breeding dog’s development. You do not want to mask the expression of dysplasia causing genes in breeding stock. Breeders should evaluate prospective breeding dogs raised under fairly uniform conditions, which neither promote, nor overly protect against hip dysplasia.
The genetic cause of hip dysplasia between these two dogs is different.
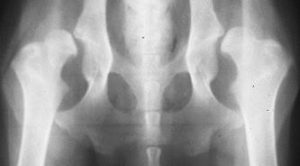 All dogs do not have hip dysplasia due to the same gene combinations. A dog with laxity and subluxation but normal anatomy has hip dysplasia caused by different genes than a dog with no subluxation but malformed sockets. Selection against the components of the syndrome may provide better control.
All dogs do not have hip dysplasia due to the same gene combinations. A dog with laxity and subluxation but normal anatomy has hip dysplasia caused by different genes than a dog with no subluxation but malformed sockets. Selection against the components of the syndrome may provide better control.  If a quality dog is to be bred, but has shallow hip sockets, it should be bred to a dog with deep hip sockets. Two dogs with fair hips can be bred together and produce much worse hips if they share detrimental traits, or could improve on each other if they compliment each other’s good traits. You need to select for enough genes influencing normal development, to get above the threshold where dysplasia develops. Not all of these aspects will insure a genetically normal dog, but the chances increase with the more that are present.
If a quality dog is to be bred, but has shallow hip sockets, it should be bred to a dog with deep hip sockets. Two dogs with fair hips can be bred together and produce much worse hips if they share detrimental traits, or could improve on each other if they compliment each other’s good traits. You need to select for enough genes influencing normal development, to get above the threshold where dysplasia develops. Not all of these aspects will insure a genetically normal dog, but the chances increase with the more that are present.
Phenotypic Tests for Hip Dysplasia Control
The Orthopedic Foundation for Animals (OFA) has a longstanding hip dysplasia registry to attempt to control the disorder based on an extended-hip radiograph. OFA ratings are based on hip joint conformation (anatomy), joint laxity, and remodeling (arthritic changes). The Institute for Genetic Disease Control (GDC) also maintains a registry for hip dysplasia based on the extended leg view.
The PennHip method of evaluating hip status is based on a measurement of joint laxity different from that recorded on the extended leg radiograph. The PennHip method utilizes a radiograph taken while applying a uniform force on the hips of an anesthetized dog to measure the maximum distractibility of the hips. By computing a breed average of distractibility, and selecting for tighter hips than the breed average, it is believed that the incidence of hip dysplasia should decrease over time.
There are pros and cons to both the OFA and PennHip radiographic methods of hip dysplasia control. The OFA radiograph documents anatomical abnormalities (shallow sockets, early bony changes), but only natural laxity in a hip extended view. The PennHip radiograph documents maximum distractibility, but many dogs with a high distraction index do not develop hip dysplasia. It is shown that both techniques have false positive and false negative results. For both methods, radiographic findings at an early age are highly correlated to dysplasia at a later age. OFA does not give permanent certification until two years of age, but offers preliminary evaluations at any age.
While PennHip identifies maximal laxity, and OFA identifies hip conformation, neither radiographic method accounts for the breadth of pedigree. For selective pressure against hip dysplasia, these tests must be used in conjunction with knowledge of the hip status of the littermates.
Selection for Breadth vs. Depth of Pedigree
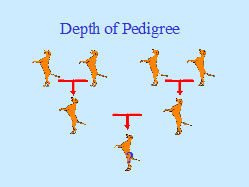 Another reason for diminished progress against hip dysplasia and other polygenic disorders is that breeders have been selecting for generations of phenotypically normal parents and grandparents (depth of pedigree). In polygenic disorders the phenotype of the full brothers and sisters more directly represent the range of genes present in the breeding individual. In other words, the breadth of the pedigree is as important, if not
Another reason for diminished progress against hip dysplasia and other polygenic disorders is that breeders have been selecting for generations of phenotypically normal parents and grandparents (depth of pedigree). In polygenic disorders the phenotype of the full brothers and sisters more directly represent the range of genes present in the breeding individual. In other words, the breadth of the pedigree is as important, if not 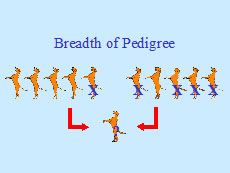 more important than the depth of the pedigree in polygenic disease control. If a dog with normal hips comes from a litter with a high incidence of hip dysplasia, you would expect it to carry a higher than normal genetic load of genes for hip dysplasia. By selecting for breadth of phenotypically normal littermates of breeding dogs, and of parents of breeding dogs, all breeds should realize a decrease in hip dysplasia. In addition, the offspring of breeding dogs should be monitored to see which are passing the disorder with higher frequency.
more important than the depth of the pedigree in polygenic disease control. If a dog with normal hips comes from a litter with a high incidence of hip dysplasia, you would expect it to carry a higher than normal genetic load of genes for hip dysplasia. By selecting for breadth of phenotypically normal littermates of breeding dogs, and of parents of breeding dogs, all breeds should realize a decrease in hip dysplasia. In addition, the offspring of breeding dogs should be monitored to see which are passing the disorder with higher frequency.
This article can be reprinted with the permission of the author: jerold.bell@tufts.edu
Leave A Comment